Reviewed by Dr. Grace Ramosena, MBChB on Jan 25, 2026
Enter at least 2 beta-hCG blood test results to estimate doubling time or halving time, compare your trend with typical early-pregnancy ranges, and view a chart.
What your results actually mean in real life
| Badge | What it usually means | Next step |
|---|---|---|
| Faster than typical | Often seen in healthy singleton or twin pregnancies | Continue routine care |
| Within typical range | Often falls within published early-pregnancy reference patterns | Schedule your dating scan |
| Slower than typical or Very slow rise | Can still be viable (15% of healthy pregnancies rise <66% in 48h), but needs watching | Repeat beta in 48h + early ultrasound |
| Declining trend | Often (but not always) indicates pregnancy loss | Contact your doctor today - they can guide next steps |
Remember: hCG is only one piece. Ultrasound is the gold standard for viability.
Looking for a different hCG calculator?
If you only have a single lab value or you’re expecting multiples, these tools are a better match than the Doubling Time (with Chart) calculator. Try Beta hCG: How Many Weeks Pregnant? or hCG Doubling Time for Twins/Triplets.
Beta hCG: How Many Weeks Pregnant?
Enter one value to see your likely week and the full typical hCG ranges by week.
hCG Doubling Time: Twins/Triplets
Calculate doubling time for multiples with a 48-hour projection and log-scale chart.
How to use this calculator
- Enter your draws: type the exact date/time and hCG value for at least two draws. Use the same lab if possible.
- Add more points (optional): click "Add another draw" to include extra results. Wider gaps of 24-48 hours are most useful.
- Set a projection (optional): choose a future date/time or leave blank to project +48 h from the last draw.
- Calculate: press Calculate to see the doubling time, a quick context badge, the projection value, and a chart.
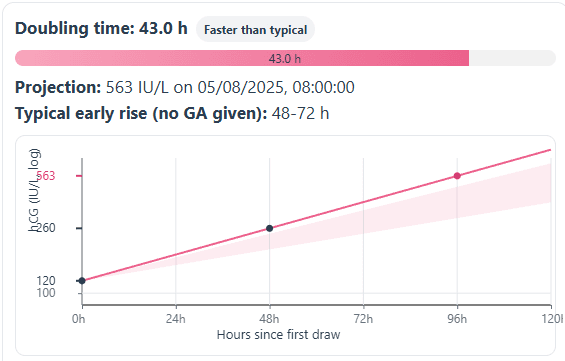
How to read the chart
- X-axis: hours since the first draw.
- Y-axis: hCG (IU/L) on a log scale, so equal vertical steps mean equal percent change.
- Shaded band: a stage-appropriate "typical" rise envelope used for comparison.
- Dark points and pink line: your measured draws and the fitted trend.
- Projection point: the predicted hCG at the chosen time. The result notes show the projected value and gestational age context when available.
- Badge and bar: classifies the rise as Faster than typical, Within typical, Slower than typical, or Declining. The bar fills more with shorter doubling times.
Educational tool only. It does not diagnose any condition and does not replace a clinician review.
hCG calculator: FAQs
How is hCG doubling time calculated?
The tool fits an exponential trend to your results. With two points it uses the exact slope. With three or more it uses a least squares line on ln(hCG) vs time. If levels fall, it shows a halving time.
What is a typical doubling time in early pregnancy?
About 48-72 h before ~6 weeks. About 72-96 h around 6-7 weeks. It can be 96-144 h after ~7 weeks. Ultrasound provides the definitive assessment.
How many draws do I need?
At least two. A third draw can smooth noise and improve the fit. Gaps of 24-48 h are the most informative.
Does a slow rise always mean something is wrong?
No. hCG is one piece of information. Some viable pregnancies rise slower. Some non-viable cases can rise faster. Trends are interpreted with timing and ultrasound.
Can I compare results from different labs or times of day?
Use the same lab when you can. Assays differ. Time-of-day effects are small compared with multi-day change, but consistency helps.
How accurate is the projection to a future date?
It assumes your recent rate continues. Biology varies. Treat the projection as a guide and follow your clinician's plan.
Why does the chart use a log scale?
hCG changes by percentages, not constant amounts. A log Y-axis turns equal percent changes into equal steps, so slopes reflect rate cleanly over wide ranges.
Methodology
Purpose of this tool
This calculator describes how quickly a series of blood hCG results is rising or falling over time. It estimates a doubling time (for rising trends) or halving time (for falling trends), then compares that value with broad reference bands for early pregnancy. It does not diagnose ectopic pregnancy, miscarriage, or trophoblastic disease.
How the doubling or halving time is calculated
The model treats early hCG change as an exponential process and uses log values:
- Sorting and cleaning: All entered draws are sorted by date and time. Only rows with a valid date, time, and positive hCG value are used.
- Log rise model: Each value is converted to the natural logarithm of hCG and plotted against hours since the first draw.
- Two draws: For exactly two points, the slope
kis the log change divided by the time gap. Doubling time isln(2) ÷ khours. - Three or more draws: For three or more points, the calculator fits a least squares line to all log values. Doubling time is again
ln(2) ÷ kusing the fitted slope. - Flat or falling values: If
kis zero within rounding, the result is reported as no rise. Ifkis negative, the tool reports a halving time instead of a doubling time.
Typical rise bands by level
The comparison bands are based on published data for serial hCG in early pregnancy and then simplified for this calculator:
- Lower hCG levels: For values below about 1,200 IU/L, a general early pregnancy band of roughly 48 to 72 hours is used for reference.
- Mid-range levels: For values between about 1,200 and 6,000 IU/L, the expected range widens to about 72 to 96 hours as rises naturally slow.
- Higher levels: Above about 6,000 IU/L, rises often slow further, so typical doubling times of about 96 to 144 hours are still compatible with uncomplicated pregnancies.
- Badge wording: The summary badge reads declining when the fitted slope is less than or equal to zero. Otherwise it classifies the trend as faster than typical, within typical, or slower than typical compared with the level-matched band.
Projection and chart
The tool can project an expected hCG value at a future date and time:
- Projection: The chosen project to time is calculated from the fitted line, starting from the last measured value. If no time is entered, the calculator uses 48 hours after the last draw.
- Chart: The chart uses a logarithmic Y axis (IU/L) and shows hours since the first draw on the X axis. A shaded band represents the stage matched typical rise envelope for visual comparison.
- Progress bar: A simple bar maps doubling or halving times between about 24 and 192 hours onto a 0 to 100 percent scale to give quick context.
Data entry tips
To make the output easier to interpret:
- Use the exact report date and time for each blood test when possible.
- Try to keep gaps between tests around 24 to 48 hours. Very short or very long intervals make trends harder to interpret.
- Later in the first trimester, natural slowing of hCG means that longer doubling times can still be normal.
Limitations
Serial hCG patterns are only one part of early pregnancy assessment. Laboratory variation, biological variation, and differences between assays can shift values. Atypical rises or falls can be seen with viable intrauterine pregnancies, early pregnancy loss, or ectopic pregnancy. This calculator does not confirm or exclude any of these conditions and is not a substitute for clinical assessment and ultrasound.
Sources we used
This hCG calculator is based on clinical guidance and research about how serum hCG changes in early pregnancy, and how trends are interpreted alongside symptoms and ultrasound.
- Hendriks E, MacNaughton H, Mackenzie MC. "First Trimester Bleeding: Evaluation and Management." American Family Physician. 2019. aafp.org.
- Anderson J, Ghaffarian KR. "Early Pregnancy Diagnosis." StatPearls. NCBI Bookshelf. ncbi.nlm.nih.gov.
- Larrain D, et al. "beta-human chorionic gonadotropin dynamics in early gestational events: a practical and updated reappraisal." Journal of Clinical Medicine. 2024. pmc.ncbi.nlm.nih.gov.
- National Institute for Health and Care Excellence (NICE). NG126: "Ectopic Pregnancy and Miscarriage: Diagnosis and Initial Management." nice.org.uk.
Support if you have experienced a loss
Reading about miscarriage, stillbirth, or infant loss can be difficult. If you have experienced a loss, you do not have to use this calculator or read the statistics. You may find it more helpful to talk with your care team or a support organization.
In the United States, groups such as:
offer information and bereavement support. If you are elsewhere, your local health service or a pregnancy and baby loss charity may be able to guide you to support in your region.
Medical disclaimer
The information and calculators on this site are educational tools only. They provide statistical estimates based on published research and the details you enter.
They cannot diagnose, predict what will happen for you, or replace personalized advice from a licensed health care professional who knows your full history. Always talk with your doctor, midwife, or other qualified clinician before making decisions about your health, fertility, or pregnancy.
Never ignore, avoid, or delay seeking professional medical advice because of something you read here or a result you see in a calculator. If you think you may be having a medical emergency, call 911 in the United States or your local emergency number.