Enter your age and optional partner or lifestyle details to estimate age-based pregnancy chances, rough time-to-pregnancy, and fertility-treatment outlooks. This is a planning estimate, not a diagnosis. It cannot measure ovulation, egg quality, sperm factors, tubal factors, or your medical history.
Pregnancy Chance per Cycle
0.00%
0.00% per random intercourseKey Fertility Metrics
This estimation does not replace professional medical advice. Always consult a healthcare provider.
How to read your fertility result
The calculator starts with age because age is one of the strongest predictors of natural fertility. It then adjusts for the optional details you enter. Read the result as a planning range, not as a personal forecast.
Chance per cycle
This is usually the most useful number on the page. It estimates the chance of pregnancy over one menstrual cycle, assuming ovulation occurs and timing is reasonably close to the fertile window.
Chance from one act of intercourse
This estimate is lower because one act may not happen near ovulation. Timing matters. ASRM describes the fertile window as the six days ending on ovulation, with the strongest timing usually in the two days before ovulation.
Time to conceive
The month estimate comes from repeated cycles. It does not mean pregnancy is expected by that exact month. Some people conceive quickly at a low estimate; others take longer at a higher estimate.
Egg count and egg quality
The egg-count line is a model estimate. It cannot tell you your actual ovarian reserve. AMH and antral follicle count can add context, but age still matters because egg quality changes with age.
IUI, IVF and egg freezing estimates
The treatment numbers are rough planning estimates. A clinic's result can be very different depending on diagnosis, medication response, sperm factors, egg source, embryo testing, and transfer details.
Fertility by age quick guide
| Age entered | How to read the result |
|---|---|
| Under 30 | Age is usually less limiting, but timing, ovulation, sperm factors and cycle regularity still matter. |
| 30-34 | Results often remain fairly strong, but this is a useful range for comparing "try now" versus "try later" scenarios. |
| 35-37 | Chance usually starts falling faster. If you have been trying for several months, the "when to seek help" result matters more. |
| 38-40 | Age becomes a larger part of the estimate. Treatment-specific calculators may give a clearer next-step view. |
| 41-44 | Natural pregnancy is still possible, but results become more sensitive to individual medical factors. |
| 45-49 | Read the result cautiously. It is mainly useful for broad planning and should not replace medical advice. |
| 50+ | The calculator keeps older hypothetical scenarios available, but it shows very low or not-estimated values where the model is not clinically reliable. |
What this calculator can and cannot tell you
It can help you compare broad scenarios, such as trying now versus later, or natural conception versus IUI, IVF, or egg freezing estimates. It cannot confirm ovulation, diagnose infertility, predict a clinic-specific IVF outcome, or account for every medical factor.
If your cycles are irregular, you have known fertility problems, you have had repeated losses, or you are over 40, a calculator result should not delay medical care. ASRM says fertility evaluation is commonly started after 12 months of trying under age 35, after 6 months at age 35 or older, and sooner when there are known risk factors.
Sources and method notes
Published guidance supports the broad age trends shown on this page. The exact pregnancy, egg-count, risk, and treatment figures are planning estimates from the calculator's model, not individual clinical predictions. Ovulation timing, sperm health, tubal factors, diagnosis, egg source, and treatment protocol can all change the result.
Key references include ASRM guidance on natural fertility and fertility evaluation, plus ACOG guidance on age and fertility. The broad egg-count trend follows the ovarian-reserve model reported by Wallace and Kelsey. The age pattern for miscarriage follows the large prospective study by Magnus and colleagues. CDC ART success-rate data provides population context for IVF, but the IUI, IVF, and egg-freezing figures shown here remain population-based planning estimates rather than clinic-specific results.
Frequently Asked Questions
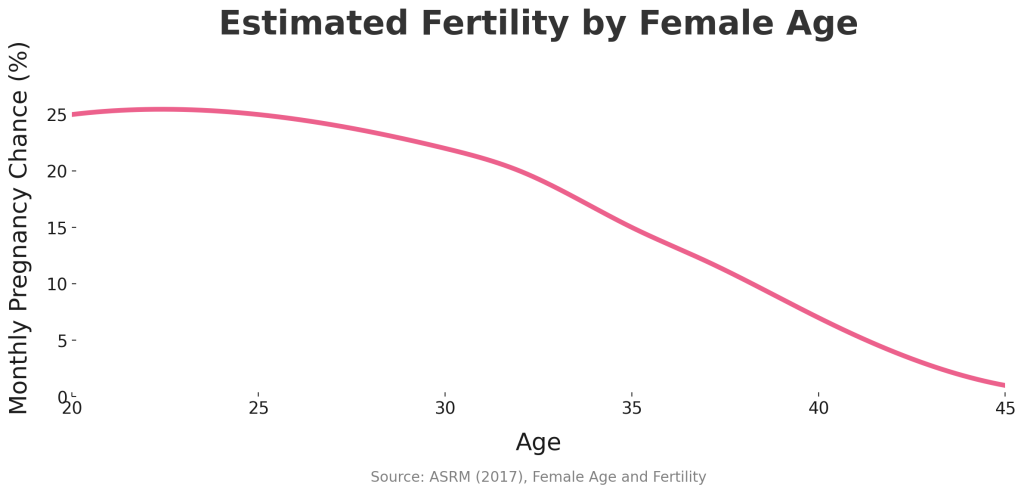
Fertility is generally highest in the 20s and early 30s, declines through the 30s, and falls more quickly in the late 30s and 40s. The percentage above is a population-based planning estimate. It cannot measure your individual egg quality, ovulation, sperm factors, or tubal factors.
It’s a screening threshold, not a cliff. Risks (lower conception odds, higher miscarriage/aneuploidy) rise gradually with age. Our model treats age as a continuum—turning 35 doesn’t halve your odds overnight.
Male age can affect fertility, but the change is usually more gradual than female age. If you enter a partner's age, the calculator uses it as one model input. The adjustment is a planning estimate, not a semen analysis or an individual prediction.
AMH reflects egg quantity, not egg quality. Quality (chromosomes) tracks strongly with age, so AMH can’t “cancel” age effects. High AMH may predict stronger IVF response; natural conception still follows age-related egg quality.
Lifestyle cannot stop egg ageing. Avoiding smoking and looking after your general health may matter, but research cannot turn those factors into a precise personal fertility increase. Lifestyle information provides context within the planning estimate.
This calculator uses an age baseline and does not predict whether or when you ovulate. With PCOS or irregular cycles, timing may vary. Ovulation tracking can add separate timing information, but it does not turn this result into an individual prediction.
No. Age-related changes in egg number and quality continue over time (ACOG). After hormonal contraception is stopped, return to fertility can vary by method; a large prospective cohort found short delays after some methods but little evidence of a lasting reduction in fecundability (Yland et al., 2020).
Not necessarily. A low age-based estimate does not identify the cause or determine one treatment path. A clinician may discuss timed intercourse, ovulation treatment, IUI, IVF, or donor eggs depending on your testing and history. Seek evaluation earlier as age rises.
The calculator shows a rough time-to-conception estimate based on its per-cycle chance. It assumes the chance stays similar from cycle to cycle, so it is not a deadline or promise. For separate 3-, 6-, and 12-month estimates, use the Conception Chance Per Month Calculator.
Under 35: after 12 months of trying. Age 35 or older: after 6 months. If you are over 40, or have irregular cycles, a known fertility factor, or recurrent loss, seek evaluation sooner rather than waiting for a fixed interval.